

By Ayele Addis Ambelu; Kule Refugee Camp, Gambella Region, Ethiopia
At dawn in Kule Refugee Camp, the dust rises before the sun. Mothers wrap shawls around feverish children. A queue forms outside a 104-bed health center before the gates even open. As they are let in, health workers in white vests unlock the outpatient department. Somewhere inside, a newborn cries. Outside, the wind carries a whisper: “When the world looks at us, we have escaped death, but death is still here.”
Kule Refugee Camp is located approximately 800 kilometers from Addis Ababa and about 40 kilometers from Gambella town. Established in May 2014 and coordinated by the Refugees and Returnees Service (RRS), the 27,000-square-metre camp sheltered more than 55,000 South Sudanese refugees as of October 2022. Around it, 59,212 host community members in the woreda and 3,736 in Terpham kebele live with the shared portion of flood, conflict, and economic strain.
Seven camps across Gambella host refugees from South Sudan. Kule is one of the largest with five schools, one health center, one clinic, and two food distribution centers. On paper, the infrastructure exists, but in reality, the needs exceed the lines drawn on maps. And yet, in this fragile geography of displacement, hope survives, in hospital wards, during vaccination campaigns, and in the steady hands of doctors who refuse to look away.
Women in the Eye of the Storm
Kule is a camp of mothers. Women outnumber men, totaling 28,091 and 23,433 respectively. Several women head households after war fractured their families in South Sudan.
Nyabol Jock sat beside her twins in the maternity ward at MSF health center. She had been hospitalized for seven days.
“They treated me well,” she said. “They stayed with me day and night.”
Nyajuok Tut also shared a similar experience, “They are with us for 24 hours doing all they can for our health.”
However, healthcare cannot replace food. A woman representative who preferred not to be named praised MSF medical services but highlighted a gap in food support which she stated undermined medical treatment offered.
“MSF is strong in health. But food support is low. When there is no food, children come back to the hospital,” she stated bluntly.
Sexual and gender-based violence (SGBV) resulted into trauma. Survivors received confidential clinical care, post-exposure prophylaxis, counseling, and referrals. An MSF mental health counselor explained: “We never ask survivors to relive trauma. We focus on recovery. Safety first. Dignity always.”
Nyajuok Tut Lual, a community representative told the reporter, “Women suffer a lot, no water, no firewood. When we go outside, we risk attack.”
Psychosocial support sessions filled small rooms daily. Trauma does not seem to end when conflict is fled. It sometime migrates with the displaced persons and refugees.
A camp at crossroads of global crisis
The world faces what experts call a “polycrisis” overlapping global emergencies. The United Nations Office for the Coordination of Humanitarian Affairs (UNOCHA) has repeatedly warned of severe funding gaps affecting food assistance, education, and protection services in displacement settings including Kule camp.
Funding cuts rippled through refugee education programs. In Kule, schools were closed due to budget shortages as children roamed the camp instead of learning.
Khur Malooth, a youth representative said, “We escaped the war and found safety. But without education, what future do we have?”
The World Food Programme (WFP) has reported rising global hunger levels due to conflict and climate variability. Food pipeline disruptions directly impact refugee rations adversely affecting feeding.
The Global Report on Food Crises (GRFC) 2026 indicates an estimated 35.5 million children affected by acute malnutrition exacerbated by displacement. In Kule, reduced food assistance has a bearing on spikes in malnutrition admissions. It is not a theory. Poor feeding translates to medical cases of a child with a fever, a mother with anemia and a malnourished toddler struggling to breathe.
According to the latest global data from the United Nations High Commissioner for Refugees (UNHCR), more than 110 million people worldwide are forcibly displaced by conflict, persecution, and climatic shocks. Ethiopia itself hosts one of Africa’s largest refugee populations.
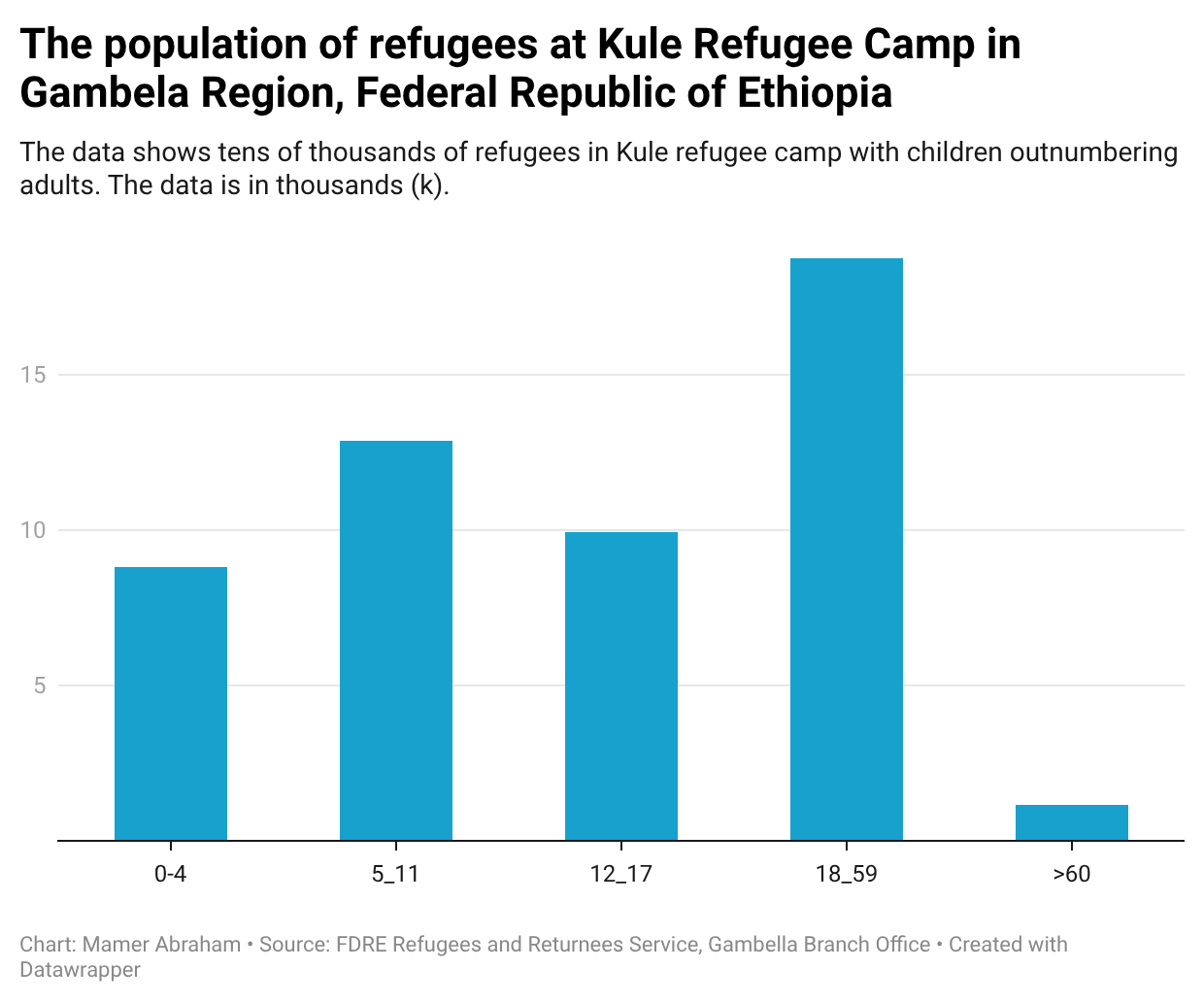
Kule’s demographic data tells its own story of vulnerability. The camp’s population includes 8,811 children aged 0–4, 12,878 children aged 5–11, 9,927 adolescents aged 12–17, 18,758 adults aged 18–59 and 1,150 elders over 60. According to this data children outnumber adults.
MSF for Medical Care
Since 2013, Médecins Sans Frontières (MSF) has provided a comprehensive care in Gambella region and moved to Kule in 2014 following the Camp’s establishment. According to the 2025 MSF Ethiopia Annual Report, Kule remains one of its most intensive operation areas in the country, responding to malaria, cholera, malnutrition, and mass casualty incidents.
Inside the104-bed capacity health center beds are rarely empty with seventy-five percent (75%) occupancy, at times higher. The corridors smell of disinfectant and boiled porridge for malnourished children.
Million Melaku, an MSF medical team leader assistant, speaks calmly but with urgency.
“We provide outpatient consultations, emergency services, surgical referrals, maternal & child health, inpatient admissions, vaccination, therapeutic feeding program for severe malnourished children under 5, chronic care (TB and HIV treatment, Snake bite, Kala Azar, etc.), WatSan & Infection & Prevention Control, health promotion, mental health and psycho-social support, treatment for survivors of sexual and gender-based violence,” Melaku explained.
MSF’s services in this camp are both primary and secondary comprising outpatient consultations, inpatient admissions, maternity care, and malnutrition treatment through an Inpatient Therapeutic Feeding Centre (ITFC), surgical referrals, mental health sessions, and Sexual Gender-Based Violence (SGBV) support.
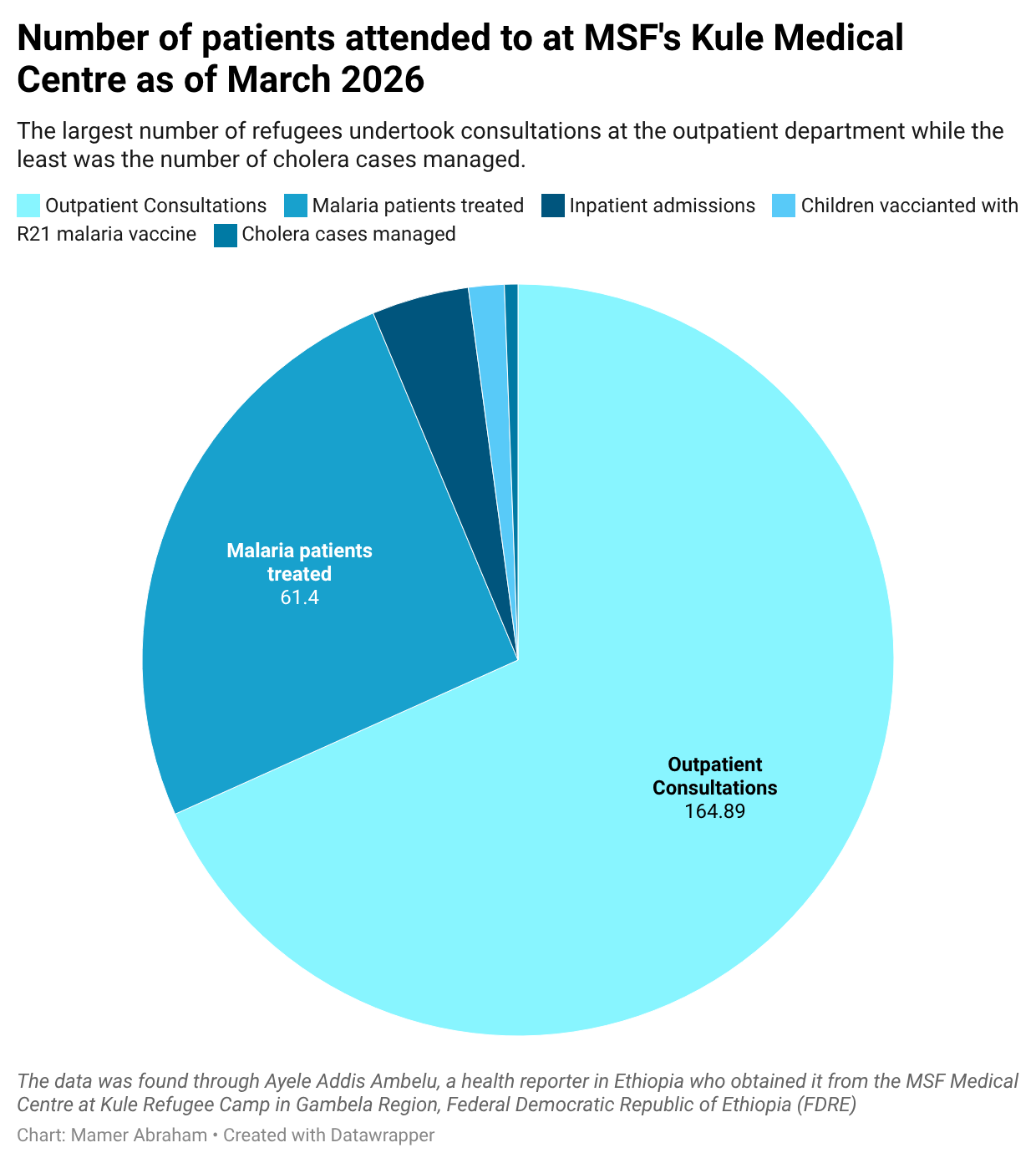
In 2025 alone at Kule, 164,886 outpatient consultations were made, 10,101 inpatient admissions executed, 61,399 malaria patients treated, 1,400 cholera cases managed, and 3,701 children vaccinated with the R21 malaria vaccine.
Game changer vaccine
One story stands as a model for global solidarity, the R21 malaria vaccination campaign. Malaria has long been a leading killer in Gambella. In 2024-2025, MSF introduced the WHO-approved R21 vaccine in Kule. By November 2025, 3,701 children received full vaccination. It was reported as the first full vaccination round completed in a refugee camp globally. Nearly 50% reduction in malaria-related deaths was recorded in 2025 compared to 2024.
This was not merely seen as a medical intervention but a game changer. The broader prevention and control efforts include vector control measures such as indoor residual spraying and environmental management, alongside community outreach activities focused on mosquito net distribution and education.
However, one doctor in the pediatric ward stated that lack of food increased admissions at the medical centre, “Most of our patients are children under five, mostly with Malaria, severe acute malnutrition or pneumonia. When food rations are delayed, admissions increase.”
The message was clear. “Even in a refugee camp, amid funding cuts, in a remote corner 817 kilometers from the capital, innovation and coordination can still save lives.”
Global Patterns, Local Realities
From Afar’s malnutrition wards to Tigray’s mental health programs and Somali Region’s emergency vaccination campaigns, MSF’s footprint across Ethiopia reveals a pattern of need layered upon needs, armed conflict, epidemics and displacement.
In Gambella, climate-induced seasonal floods and conflict continue to isolate communities. Malaria surges with rising temperatures. Cholera follows contaminated water. MSF has employed about 1,500 local personnel in Ethiopia. Many cross conflict lines and hard to reach areas to treat patients.
An MSF nurse told me calmly, “We do not choose sides. We care for everyone who needs us.”
Founded in 1971 and awarded the Nobel Peace Prize in 1999, MSF operates under the principles of Medical Ethics, neutrality, independence, and impartiality.
“What One Message Should the World Hear?” I asked this closing question to every interviewee.
Nyakoch Riek, women representative, answered: “Do not forget us. We did not choose to leave our homes.”
Khur Malooth said, “Education is as important as food.”
Million Melaku stated, “Sustained funding. Without it, the burden doubles.”
Mr. Khan added, “Support both refugees and host communities.”
An anonymous survivor of violence whispered through a counselor: “Support saved my life.”
Wiyual Gach, an elder, reflected: “We pray every day to return home. But peace is not coming. Our hope is not real yet.”
The world is at crossroads, global displacement rising, climatic shocks intensifying and humanitarian budgets shrinking, yet in Kule, a camp in western Ethiopia, doctors dress hope in a white coat, administer vaccines, transfuse blood and deliver counseling for trauma healing.
The story of resilience of over 55,000 refugees surviving in land not their own reverberates and the warning that if solidarity fails, refugees living in camps like Kule will bear the cost.
As the sun sets over Gambella’s plains, mothers still line up outside the clinic. Children still cough in the dust. Elders still pray for return. And somewhere inside the health center, a newborn takes the first breath. The world may be torn between hope and disaster. But in Kule, the choice is made as the clock ticks, revitalizing firmness to save lives, and reviving hope.